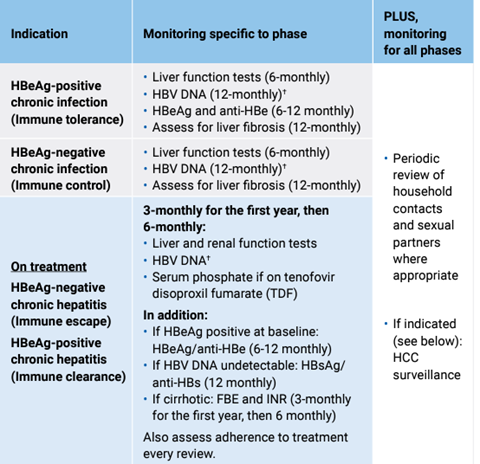
For information on assessing whether or not a person requires medication see the hepatitis B decision making tool.
Medications for hepatitis B on the PBS include entecavir and tenofovir. These can only be initiated and prescribed by an accredited hepatitis B community s100 prescriber or a tertiary specialist.
There is a provision for GPs to prescribe maintenance therapy when it is impractical to get a prescription from the treating affiliated specialist medical practitioner and the specialist has agreed to the prescription. For more information see here.
For information on hepatitis B and pregnancy see here.
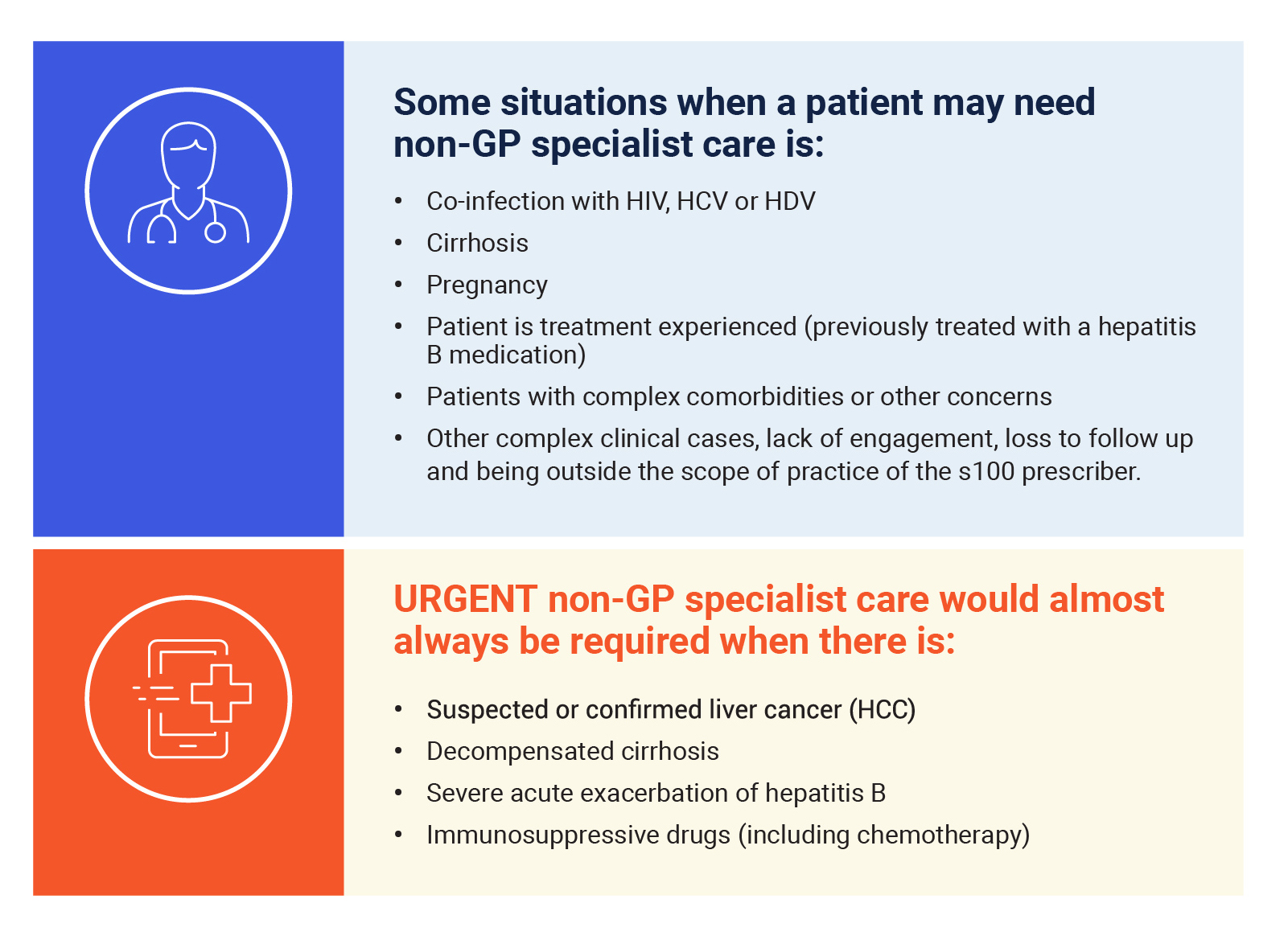
Co-infection with HIV, HCV or HDV. For information on co-infection see here.
For guidance on where to refer your patient see here.
Local information regarding referral can be found on HealthPathways. For further information and links to location-specific HealthPathways in Victoria see here.